The steps are: planning, installation, surgical approach, acetabular exposure and the establishment of the acetabular implant, exposure and the establishment of the femoral stem, testing stability and length and closing..
Planning :
This is provided the size and positioning of the prosthesis according to the morphology of each patient. It postpones layer on radiographs according to specific criteria. This is done in the operating room.
Installation :
Once anesthesia is achieved either regional loco is complete, the patient is placed on the operating table.
For one channel lateral or posterior approach, the patient is placed on the side held by presses of the buttock and the pubis.
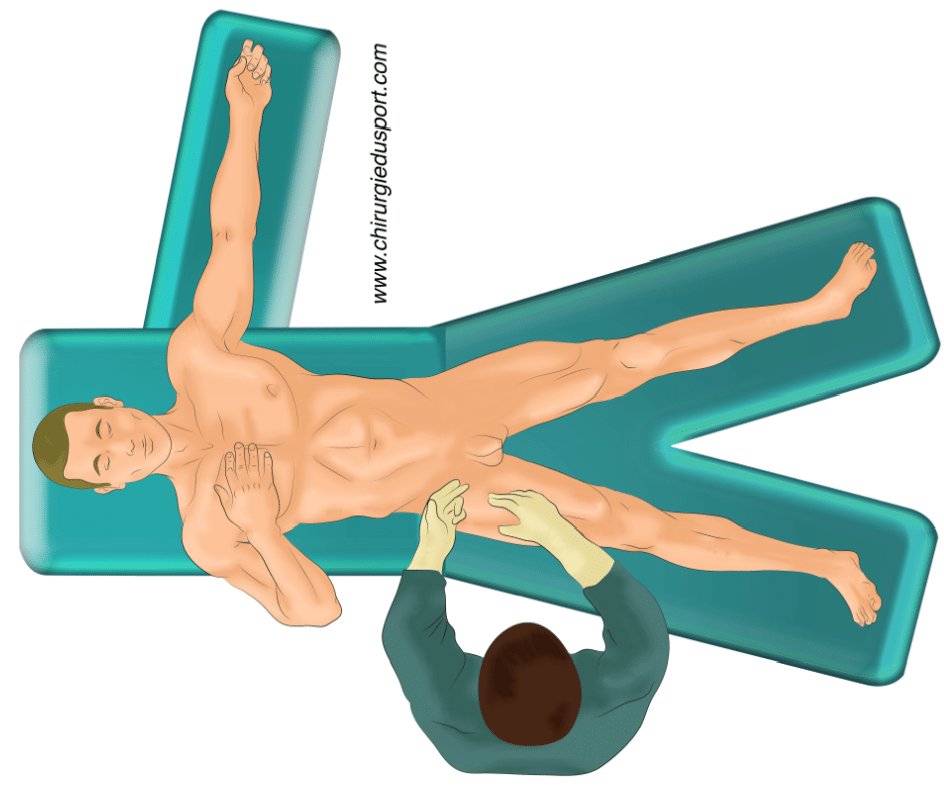
For an anterior approach, this requires a special table called “orthopedic” for the operated limb is placed in a boot for applying traction (Fig 1).
The patient’s skin is then prepared by repeatedly antiseptic washes before operating aid set up drapes that separate the scar area.
The way first :
The hip joint is a very deep access to which requires a strategy that initially affects the installation, types of implants used and the postoperative. There are three main approaches: posterior, lateral and anterior. Each technique has advantages and disadvantages.
The exposure of the acetabulum and implant :
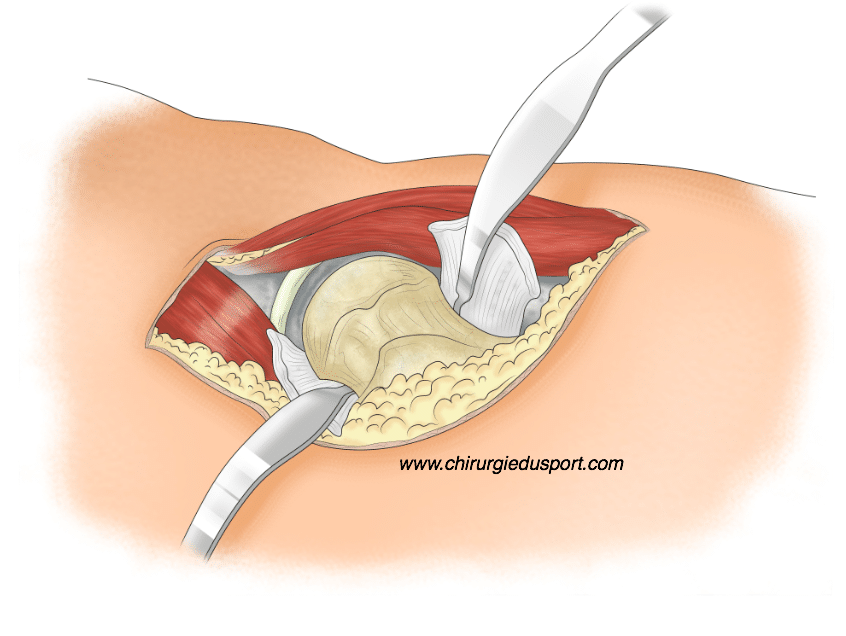
Once the affected joint, the femoral neck cut is madeEither before or after dislocation of the joint (Figure 2). This section is very important because it determines the vertical position and in front of the rod, which is then implanted. We identify the anatomical elements of the acetabulum (rear bottom, front and back edges, obturator foramen). The rest of the cartilage is removed with a motorized ball milling the size of the planned implant. Then, the final implant is fixed either with cement or by impaction in the basin.
The exposure of the acetabulum and implant :
This is exposing the upper end of the femur that has been cut. Rods in forms of increasing size rasps are progressively impacted in the cavity of the femur until a rod is adapted perfectly to the femur size. Then, the implant defines femoral set either with cement or by impaction.
The intraoperative examination of the length and stability of the prosthesis or “testing”:Once the hip is reduced, ie, it is resocketed (reduced) with implants, it is verified that the planned length is respected. There is the possibility at the time of increasing or reducing this length with ball of the femoral head sizes. Then the stability of the hip is tested by mobilizing the extreme situation to ensure that it is not luxury (flexion and extension internal rotation external rotation).
The closure :
is then, after joint lavage, the suture different plans according to the open surgical approach used.Post-operative care involve scar care, anticoagulation therapy, rehabilitation and regular visits in consultation.
Doctor Yoann BOHU, Doctor Serge HERMAN. – 1 novembre 2013