Introduction:
Meniscal injuries athlete are frequent. These lesions should be properly diagnosed and treated. The treatment is no longer based on the simple meniscectomy may be the cause of cartilage changes over time. The term goal is to preserve the cartilage in this young athletic population and submitting his knees major constraints, priority should be given the meniscal economy (suture or abstention).
It is important to distinguish traumatic meniscal lesions of degenerative meniscal lesions. Traumatic injuries occur in young patients under 35 years with initial concept of trauma or repetitive strain injuries; while degenerative meniscal lesions affect an older population (35/50 years) without any trigger. This distinction is schematic and is not always so clear. Nevertheless it helps guide us in choosing the treatment of meniscal lesions.
Physiological reminder:
The menisci are triangular fibrocartilage semilunar the cut. They have a bone anchored by their anterior and posterior horns, related to pre- and retro-spinal surfaces and capsular ligament anchors the circumferential peripheral edge. The meniscus is only partially vascularized. Vascularisation from a capsular arterial plexus that enters the meniscal thickness from the capsule about 20% of the width meniscus (Figure 1). He receives another vascularization from the bone insertion of horns. This peripheral vasculature supports the healing of cracks in “red red” zone.
The meniscus is composed essentially of water (75%) and an extra-cellular matrix (25%): it is mainly composed of type I collagen (90%), proteoglycans and non-collagenous proteins. The type I collagen comes together in bundles that align differently in size and depth. This configuration, radial and circumferential, form an optimal construction for the damping function (Figure 2).
When walking or during the axial load, the structure allows the menisci by alternating the charge / discharge to create a continuous lubrication of the surfaces. It is also thanks to the viscoelasticity of complex meniscus cartilage-that the bearing surface thus bringing increases brutal excessive charges at physiological levels.
The menisci have a role in the transmission and distribution of 50 to 70% of the constraints. They increase joint congruency and stabilization of the knee, they provide shock absorption, protection of cartilage, and finally they participate in joint lubrication.
The preservation of capital is fundamental meniscal and articular prevents degradation
Meniscal injuries
They are due to trauma
- or by excessive load on a normal meniscus
- or by physiological strength of abnormal meniscus (degenerative).
Injuries
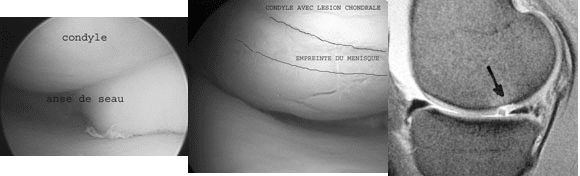
The circumferential lesions are due to rotational forces. They are often accompanied by ligament injuries. The meniscus is subject to a charge circumferential force of a vertical peripheral lesion sometimes bucket handle. (Figure 3). Sometimes the initial trauma causes concomitant chondral lesions (Figure 4) or secondary (Figure 5) by passing the bucket handle on the condyle.
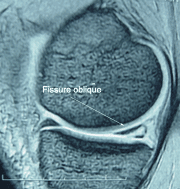
The horizontal lesions are the result of sliding forces. The concept of initial trauma may be missed.
parrot beak injuries are secondary to a torsion-compression trauma, which induces lesions of the posterior segment of the medial meniscus. They are progressive and can remain asymptomatic for a long time.
The microtrauma injuries
These lesions are induced by repetitive strain injuries. They sit at the physiological load zones, namely the posterior segment of the medial meniscus. Vertical lesions are secondary to the forces that cause rotation meniscus hypermobility and degenerative lesions. Intracorporéales the lesions are secondary to shear forces, often seated in the posterior segment of the medial meniscus. These lesions do not heal and lead ineluctably progressive degeneration. These meniscal tears in the process of degeneration induced by their irregularities impaired wearer cartilage.
Treatment of meniscal tears
The meniscal tear is not “synonymous” with meniscectomy. The partial meniscectomy is not a benign procedure. It can lead to cartilage degeneration and in osteoarthritis. We must try to preserve capital by meniscal no treatment or a meniscal suture. Their treatment depends on the type of injury, location and association with a possible ligament laxity. Still, meniscectomy remains the treatment of choice for most lesions.
We distinguish meniscal lesions on steady knee on those unstable knee.
Unstable knee

Meniscal injuries associated with knee laxity is most often represented by a peripheral avulsion of the posterior segment of the medial meniscus, despite their potential for spontaneous healing, they must be diagnosed and treated especially in children and the young athlete. Arthroscopy is used to evaluate the type of injury, an element that determines the therapeutic attitude. Injury single device or bucket handle (dislocated or not) will be sutured. A more complex lesions including combining a horizontal cleavage or a meniscal tab disinsertion be resected. Arthroscopy allows to also evaluate the size and stability of the lesion. The meniscus must be sutured, if the lesion is> 10 mm, or can be mobilized in the condyle. Otherwise, a simple denudation of the lesion enough to allow healing.
In chronic anterior laxity with meniscal lesion recent, it is desirable to achieve at the same time operating a ligament reconstruction with meniscal repair. An isolated meniscal suture is doomed to failure.
Stable knee
Meniscal lesions are rarely steady knee peripheral disinsertions. Conservation meniscus suture is more random. The goal of treatment is to preserve the long-term cartilage. Simple vertical lesions or bucket-handle must be sutured if the meniscus is healthy. We must prevent the patient’s risk of failure. An additional suture or partial meniscectomy may be indicated secondarily. We must push on indications in children and young athletes and for injuries of the lateral meniscus.
Meniscal suture
Whichever technique (open or arthroscopic sky) and the attachment method used (son or ties) should always sharpen the crack to suture on both sides to find a meniscal tissue vascularized. We must achieve a strong repair, which involves a close suture (5mm).
The prognosis of a meniscal repair depends on several factors:
- Patient age (better in children than adults)
- The age of the lesion (more favorable if <3 months)
- The state of the anterior cruciate ligament (ACL rupture more favorable if associated)
- The location of the lesion (favorable zone “red-red”).
A review of the literature shows that meniscal repair after healing is achieved in 70% of cases on knee stable and in 90% of cases if there is a torn ACL reconstructed at the same time. The lack of ligament repair is a poor prognosis factor in wound healing. The meniscal repair protects the long term cartilage as shown by the results of different runs.
Many techniques are possible:
Technical “out-in” from outside to inside. It is intended for anterior segment, access to the posterior meniscal segment is sometimes difficult.
Technical “in-out” from within outward. It allows access to posterior and middle segments with a posterior incision against. Its realization subject to the risk of neurovascular injury.
- Technique “all-inside” while there. Suture “all arthroscopic” can be achieved with a lot of new material from meniscal repair: arrows, bolts, harpoons, etc.
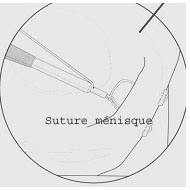
- The technique is relatively easy but with a risk of cartilage damage by direct projection equipment, and synovitis secondary to the presence of foreign body. Many biomechanical studies show the superiority of traditional direct sutures. This is why new systems are currently available to enable a suture wire with a technique “all arthroscopic”. The FasT Fix such a device is under arthroscopic control to perform a suture thread with a self-locking sliding knot (Figures 6 and 7).
Conclusion
The knee of the sport is frequently traumatized. The meniscal economy is the keyword to preserve the future of knee cartilage.
If a meniscal lesion is associated with a ruptured anterior cruciate ligament, the meniscus must be kept by abstention or a meniscal repair. Ligament repair is performed in the same operation. In the case of a meniscal lesion on a stable knee, push the indications in children and young athletes.
Doctor Nicolas LEFEVRE, Doctor Yoann BOHU, Doctor Serge HERMAN. – 28 janvier 2014.