The contribution of new imaging techniques (MRI and 3D MRI diffusion cube) and measurement of laxity (GNRB and TELOS) on the management of partial tears and isolated ACL (surgery versus conservative treatment)
Introduction
The Anterior Cruciate Ligament (ACL) of the knee consists of two anatomically and functionally distinct bundles [1,2], named according to their tibial insertion area, one anteromedial (AM), the other posterolateral ( PL). The ACL tears are common with a reported incidence of 8.1 / 100 000 per year. [3] Partial ruptures represent 10 to 28% [4] of all ACL injuries. This figure is probably an underestimate because on one hand these figures are for surgical patients, and also the definition of a partial rupture is not consensual, from the authors of the insertion easy bleeding femoral ACL to total rupture of one of the two beams. [5] Although the prognosis of partial tears is better than that of total breakdown, an unrecognized partial rupture can progress to total rupture or chronic knee instability [6] source of osteoarthritis. This risk increases with the proportion of broken fibers. The therapeutic management of the patient with a partial ACL tear is different from the total rupture. [4] On one hand, several studies have shown that long-term results of the Conservative treatment was better in case of partial tears [7,8]. On the other hand, in case of surgical repair a partial tear, this one is not on anatomical the broken beam and respecting the remaining ligament [9], which restores stability, function [10,11] and proprioception of the knee [12].
The conventional MRI showed in the diagnosis of total rupture a sensitivity of 92-96% and a specificity of 92-98% [13], accuracy in the diagnosis of partial tears is low. [14] In the absence of a reliable preoperative diagnosis on the relevant beam and the proportion of broken fibers, the partial repair of the ACL decision is often taken in Intraoperative. Improved diagnostic performance of imaging tools for partial ACL tears is a real therapeutic challenge. The contribution of new imaging technology (MRI 3D cube and diffusion MRI) and dynamic measurement tools knee laxity (telos and GNRB) have improved the sensitivity and specificity of diagnosis ruptures LCAE . Thus taking into orthopedic surgical or therapeutic treatment is better defined.
MRI or MRI Cube 3D Isotropic-ESF
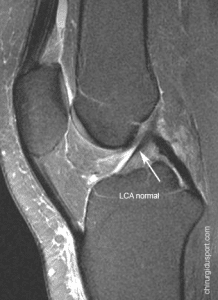
The 3D-MRI Isotropic-FSE (Fast Spin Echo) -Cube is a recent sequence validated in neuroimaging and used recently in musculoskeletal imaging [15,16], especially the [17] knee. Its accuracy is sub-millimeter. MRI 3D cube replacing multiple 2D acquisitions cup by cup, shot by shot, by a single 3D acquisition where a shorter completion time.It allows for volume acquisitions on the knee and MPR reconstructions (Multi Planar Reformation) almost immediate as the desired axes.
A retrospective study [18] evaluated the results of MRI 3D cube for patients operated a torn ACL in Sport Surgery service. The main objective this study was to evaluate the performance parameters of the 3D-FSE-Cube MRI compared to per-arthroscopic findings considered the gold standard in the diagnosis of partial ACL tears. All patients underwent preoperative MRI, conventional 2D-January 2008 to October 2009 and 3D-Cube from November to December 2009. The diagnosis of partial rupture was based on MRI appearance of ligament and beams signal quality, and arthroscopy on the continuity of the beams and the quality of the remaining ligament. Among 312 patients included, 64 consecutive patients underwent an MRI 3D-Cube and 248 of a conventional 2D MRI. Arthroscopy has found no normal ACL, 247/312 (79.2%) complete ruptures and 65/312 (20.8%) partial tears that 50/65 (76.9%) and anterior-medial 15 / 65 (23.1%) posterolateral.
Cube 3D-MRI of performance parameters for the diagnosis of partial rupture were: sensitivity 95% = 62.5 ± 23.7%, specificity 95% = 93.7 ± 6.9%, those of 2D-conventional MRI were: sensitivity 95% CI = 10.2 ± 8.5%, specificity 95% = 96.5 ± 2.5%. This study showed that in the diagnosis of partial ACL tears, the Cube 3D-MRI had a very good specificity, high sensitivity and a positive likelihood ratio of major. Its diagnostic performance was better than that of conventional 2D-MRI. The likelihood of a positive test was 9.9 times higher in patients with a partial tear. Its negativity does not allow to exclude this diagnosis with certainty. This examination: MRI 3D cube is now routinely used in the clinic of the sport in Paris in the balance sheet ruptures LCAE.
MRI diffusion
One study evaluated the value of MRI diffusion [19] in the diagnosis of complete or partial ACL tears. A conventional MRI, the diagnosis of partial or complete ACL tear is based on the appearance of ligament beams and signal quality. Diffusion MRI images were obtained with an MRI1.5-Tesla Siemens system, which is generally used for visceral imagery. Patients were placed in the same position as for a normal MRI. The images were obtained in the sagittal and transverse planes in identical positions used in the T2 sequences. It has been used a technique of spectral fat saturation. Eighty-five patients (35 women and 50 men, average age 34.1 years) with a recent knee injury (<4 months) with a suspected lesion of the LCA underwent conventional MRI (T1 and T2-weighted images with fat saturation) associated with MRI diffusion. For the diagnosis of complete rupture of the ACL (67 patients) and partial (18 patients), the sensitivity and specificity were 87% and 50% respectively with conventional MRI, and 96% and 94% respectively, with MRI diffusion (P <0.01 for specificity). The authors conclude that MRI diffusion associated with conventional MRI is a reproducible method to better differentiated complete and partial ACL tears. The same group [20] in another study evaluatedthe possibilities of healing by conservative treatment of partial tears of the anterior cruciate ligament (ACL) without moving the ligament fibers. An MRI Broadcast has selected 29 cases of recent partial ACL tears (14 women, 15 men, aged between 18 and 59 years, mean 38.8 years; average time between injury and diagnosis: 10.7 days ). MRI diffusion sequences have clarified the persistence of continuous ligamentous fibers in the post-traumatic edema. For 6 weeks, knees were immobilized by a brace with limited flexion between 30 ° and 60 ° (stored support). After 6 weeks, clinical monitoring and MRI verified the ligament continuity. Progressive knee rehabilitation was then begun. After 1 year, 28 patients (96.6%) had complete healing of the ACL with a full anatomical restoration on remote MRI. 26 patients (89.7%) had a normal ligament clinical examination (objective IKDC ligament: 17 Stage A, 9 B stage) and two patients had residual clinical laxity with hard stop (stage C). The average TELOS is rated at 2.5 mm (-1 to 8 mm) 8 months after the trauma, the weighted average subjective IKDC 92.2 (67.9 to 100) with a mean of 1 year and 11 months . The only failure was treated by ligament. The authors conclude that the diagnosis of partial ACL tears made by an MRI Broadcast, allows us to offer reliably orthopedic treatment with a high rate of healinganatomical and functional ligament.
GNRB and TELOS
The diagnosis of ruptured anterior cruciate ligament (ACL) is clinical. The meta-analysis of Solomon et al [21] showed that the diagnostic test Lachman was the most reliable, followed by the anterior drawer test and the pivot shift test. Nevertheless, objective quantification of the anterior tibial translation is a decision support tool for the surgeon both during the patient’s initial management as for the monitoring. [22] Preoperative differential laxity also gives an indication of the full or partial nature of the break. In case of partial rupture, the therapeutic issue is certain since the conservative treatment can be considered with good long-term results [23,24,25].
Several arthromètres are available [1]. The KT-1000 ™ (MEDmetric®, San Diego, USA) [26] is the most widely used because simple to use. The Rolimeter ™ (Aircast, Summit, USA) is as reliable as the KT-1000 ™ [27,28], but both are examiner-dependent. The Telos ray ™ (Gmbh, Hungen / Obbornhafen, Germany) seems more accurate than the KT-1000 ™ [29]. However this device is expensive and radiating but widely used in Europe preoperatively. The system GNRB® (Genourob, Laval, France) showed better reproducibility than the KT-1000 ™ and whatever the level of training of the examiner [30,31].
A study compared the performance of GNRB that of Telos ® and ™ in the diagnosis of a partial tear of the anterior cruciate ligament (ACL). [32] It was prospective study of all patients with partial or complete ACL rupture with or without anterior reconstruction with a healthy contralateral knee. The anterior laxity was measured in all patients by the Télos ™ and GNRB ®. The series consisted of 139 patients, mean age 30.7 ± 9.3 years. Arthroscopic reconstruction was performed in 109 patients, 97 for a complete break and 12 uni-fascicular reconstructions for a partial rupture. 30 patients with partial rupture were treated conservatively. Pathological laxity are differential thresholds according to the literature 3 mm for the KT-1000 ™ [26,33], 3 mm for the GNRB ® [31] and 5 mm for the Télos ™ [34]. There was a highly significant difference between the differential laxity of total and partial tears with both exams and whatever coercion. The optimal threshold differential laxity with GNRB ®250N was 2.5 mm (Se = 84%, Sp = 81%).
This study also identified a differential laxity threshold in partial ACL tears with Telos ™. With a force of 250N, the threshold was 3.6 mm with good sensitivity (81.5%) but an average specificity (59.5%) exposing a greater number of false positives. The authors conclude a diagnostic performance GNRB ® is better than that of Télos ™ in Partial ACL tears.
Conclusion:
Improved diagnostic performance of imaging tools for partial ACL tears is a real therapeutic challenge. The contribution of new imaging technology (3D MRI and diffusion MRI cube) and dynamic measurement tools knee laxity (telos and GNRB) have improved the sensitivity and specificity of the diagnosis of partial tears of LCAE. Thus taking into orthopedic surgical or therapeutic treatment is better defined. The surgical decisionbut is of course clinical diagnostic support for these additional examinations seems to be an asset in support of ruptures LCAE in 2015.
Bibliography
1) Duthon VB, C Barea, Abrassart S et al (2006) Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 14: 204-213
2) MT Gabriel, EK Wong, Woo SL et al (2004) Distribution of in situ strength in the anterior cruciate ligament in response to rotatory loads. J Orthop Res 22: 85-89
3) RA Clayton, Court-Brown CM (2008) The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury 39: 1338-1344
4) Umans H, O Wimpfheimer, Haramati N et al (1995) Diagnosis of partial tears of the anterior cruciate ligament of the knee: value of MR imaging. Am J Roentgenol 165: 893-897
5) J. DeFranco, Bach BR Jr (2009) A comprehensive review of partial anterior cruciate ligament tears. J Bone Joint Surg Am 91: 198-208
6) Messner K, Maletius W (1999) Eighteen- to twenty-five-year follow-up after-acute partial anterior cruciate ligament rupture. Am J Sports Med 27: 455-459
7) Ng AW, Griffith JF, Hung EH et al (2012) MRI diagnosis of ACL tears bundle: value of oblique axial imaging. Skelet Radiol.
8) Ohsawa T, Kimura M, Y Kobayashi et al (2012) Evaluation of Arthroscopic ligament remnant preserved after-selective anterior medial or posterolateral bundle anterior cruciate ligamentreconstruction. Arthroscopy.
9) Ravey JN, Dubois C, Pittet L-Barbier (2010) bi-fascicular LCAE Analysis of MRI and application to partial tears. The Sports Trauma Imaging GETROA-GEL OPUS XXXVII Sauramps Medical, Paris
10) Oldrini G, PG Teixeira, A Song et al (2012) MRI appearance of the distal insertion of the anterior cruciate ligament of the knee: an additional criterion for ligament ruptures. Skelet Radiol.
11) H Steckel, Vadala G, Davis D et al (2006) 2D and 3D 3-tesla magnetic resonance imaging of the double-bundle anterior cruciate ligament structure in anatomy. Knee Surg Sports Traumatol Arthrosc 14: 1151-1158
12) Chouteau J, R Testa, Viste A et al (2012) Knee rotational laxity and proprioceptive function 2 Years After partial ACL recon- struction. Knee Surg Sports Traumatol Arthrosc 20: 762-766
13) H Steckel, Vadala G, Davis D et al (2007) 3-T MR imaging of partial ACL tears: a cadaver study. Knee Surg Sports Traumatol Arthrosc 15: 1066-1071
14) Van Dyck P, De Smet E, Veryser J et al (2012) Partial tear of the anterior cruciate ligament of the knee: injury patterns on MR imaging. Knee Surg Sports Traumatol Arthrosc 20: 256-261
15) KJ Stevens, Wallace CG, Chen W et al (2011) Imaging of the wrist at 1.5 Tesla using isotropic three-dimensional fast spin echo cube. J Magn Reson Imag 33: 908-915
16) Tjoumakaris FP, Donegan DJ, Sekiya JK (2011) Partial tears of the anterior cruciate ligament: diagnosis and treatment. Am J Orthop (Belle Mead NJ) 40: 92-97
17) Kijowski R, Gold GE (2011) Routine 3D magnetic resonance imaging of joints. J Magn Reson Imag 33: 758-771
18) N Lefevre, JF Naouri, Bohu Y, Klouche S, Herman S. Partial tears of the anterior cruciate ligament: diagnostic performance of isotropic three-dimensional fast spin echo (FSE-Cube 3D) MRI.Eur J Orthop Surg Traumatol. 2014 January; 24 (1): 85-91.
19) Delin C, S Silvera, Coste J, Thelen P, N Lefevre, Ehkirch FP, The Couls V Oudjit A, C Radier, Legmann P. Reliability and diagnostic accuracy of qualitative assessment of diffusion-weighted MRI combined with conventional MRI in Differentiating entre full and partial anterior cruciate ligament tearsJournal Eur Radiol 2012 Aug 19
20) C Delin, S Silvera, JY Vandensteene, P Javoy, P Thelen, P Djian, D Rousseau, C Radier, P Legmann Conservative treatment of partial ACL tears. Prospective study on wound healing conducted ACL in patients selected by MRI diffusion. 25 th Congress of Rheumatology 9-12 December 2012 Paris http://poster.rhumatologie.asso.fr/ModuleConsultationPoster/consultationPoster.aspx?intIdPoster=2459
21) AJ Schuster, J. McNicholas, Wachtl SW et al (2004) A new mechanical testing device for measuring anteroposterior knee laxity. Am J Sports Med 32: 1731-1735
22) J Berry, Kramer K, J Binkley et al (1999) Error Estimates in novice and expert raters for the KT-1000 arthrometer. J Orthop Sports Phys Ther 29: 49-55
23) Bak K, Scavenius M, S Hansen et al (1997) Isolated partial rupture of the anterior cruciate ligament. Long-term follow-up of 56 squares. Knee Surg Sports Traumatol Arthrosc 5: 66-71
24) Barrack RL, SL Buckley, Bruckner JD et al (1990) Partial versus full acute anterior cruciate ligament tears. The results of nonoperative treatment. J Bone Joint Surg Br 72: 622-624
25) Branch TP Mayr HO, Browne JE et al (2010) exam- ination Instrumented of anterior cruciate ligament injuries: Minimizing manual flaws of the clinical examination. Arthroscopy 26: 997-1004
26) P Colombet, Dejour D Panisset JC et al (2010) Current concept of partial anterior cruciate ligament ruptures. Orthop Traumatol Surg Res 96: S109-S118
27) J. DeFranco, Bach BR (2009) A comprehensive review of partial anterior cruciate ligament tears. J Bone Joint Surg Am 91: 198-208
28) Robert H New S, S Gageot, Gagnie`re B (2009) A new knee arthrometer, the GNRB: experience in full and partial ACL tears. Orthop Surg Traumatol Res 95: 171-176
29) Huber FE, Irrgang JJ, C Harner, Lephart S (1997) Intratester intertester and reliability of the KT-1000 arthrometer in the assess- ment of posterior laxity of the knee. Am J Sports Med 25: 479-482
30) Buckley SL, Barrack RL, Alexander AH (1989) The natural history of conservatively biased Treated anterior cruciate ligament tears. Am J Sports Med 17: 221-225
31) L Pugh, R Mascarenhas, Arneja S et al (2009) Current concepts in knee-instrumented laxity testing. Am J Sports Med 37 (1): 199-210
32)Lefevre N, Y Bohu, JF Naouri, Klouche S, H erman S Validity of GNRB (®) arthrometer Compared To Telos ™ in the assessment of partial anterior cruciate ligament tears. Knee Surg Sports Traumatol Arthrosc. 2014 Feb; 22 (2): 285-90.
33) Bach BR, Warren RF, Flynn WM et al (1990) Evaluation of Arthrometric knees That torn anterior cruciate-have a ligament. J Bone Joint Surg Am 72: 1299-1306
34) Solomon DH, Simel DL, Bates DW et al (2001) The rational clinical examination. Does this patient-have a torn meniscus or ligament of the knee? Value of the physical examination. JAMA 286: 1610-1620
Doctor Nicolas LEFEVRE, Doctor Yoann BOHU, Doctor Antoine GEROMETTA, Doctor Serge HERMAN. – 21 octobre 2015.