Anatomy
A ligament is a fibrous cord that connects two bones together at a joint. He guides and controls its movement … until the amplitude exceeds the limits of its elasticity and this is the sprain! The ligament is different from a muscle tendon which clings to a bone to transmit its force of contraction. To fulfill its mission, the second must be more rigid! Remember well that concept! It is not intended for your general knowledge! It will serve you well to understand your operative! Your surgeon has replaced your broken by a tendon ligament … That will have some practical consequences!
It is past you!
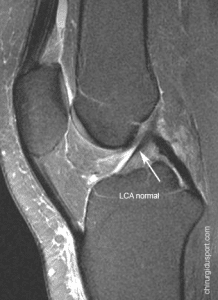
The anterior cruciate ligament lies in the knee center. It is “prior” because it fits to the front of the tibia, the leg bones. It goes to the back of the femur, the thigh bone. It is “crossed” as it crosses its path his colleague, the posterior cruciate ligament.
It limits the advance of the tibia. It also puts pressure when the knee turns or flip. You can break your “crossed earlier” when your ski spatulas depart or cross inexorably. It also rips when your knee rotates violently during a support change. This may be the case when your soccer cleats stuck in the grass or when a advesaire takle you … awkwardly!
The operation is it mandatory?
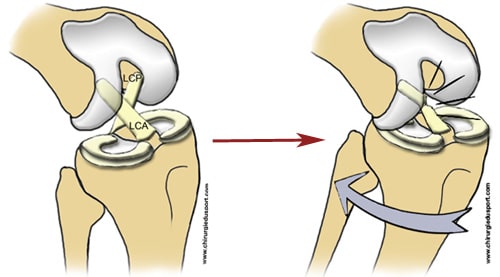
The anterior cruciate ligament is not part of the “capsule”, the bag entourrant the joint. It is isolated in the middle of the knee, with his colleague, the “posterior cross.” When it is completely broken, it does not receive any support and falls to the shin. Both ends are no longer in contact. The spontaneous healing is impossible.


However, you have heard of spontaneous healing after anterior cruciate rupture. That is true ! Well almost ! The case of Anthony Réveillère, football player at Olympique Lyonnais, hit the headlines. The ligament may have suffered a partial rupture. It is distended but remains continuous. It can repair tighten see as is the case in a routine ankle sprain. It is also possible that the anterior cruciate hangs during its fall on the posterior cruciate. Healed in this abnormal position, it sometimes helps to limited abnormal movements of the knee.
Anyway, this development is uncommon and rarely allows to obtain a perfectly stable knee, especially if you intensively practice disciplines with pivots and contacts! However, if you give up these activities to practice only sports in the axis like running and cycling, it is possible to avoid intervention. Intensive rehabilitation and medical supervision is required. It will check if the knee slips away again … and consider the operation.
Fortunately, progress has been!
It used to be sutured both ends of the cruciate ligament. Unfortunately, they were frayed like a piece of steak with shallots. Their blood vessels were shredded. Repair could not hold, the healing could not happen. The ligament die if nécrosait. Later, we realized that it was rotational instability that bothered him injured. Dr. Lemaire has to bridge a transaction which placed an anterior cruciate tendon parallel to but outside of the knee. The procedure was simple and installation of the lever arm proved to be very effective to prevent sprains in rotations. Unfortunately, the rear moves forward continued insidiously. The knee and rubbed was wearing, were damaging to the menisci.
Please replace the cruciate ligament!
Now, your surgeon removes a portion of the tendon near your knee. Either it takes one or two fine tendons located on the inside of the knee, or it uses the center part of the patellar tendon below the kneecap. The first technique is called hamstring tendons because those are the muscles Internal Law and Demi Tendinous. The second is called “Kenneth Jones” or KJ or ligament patellar tendon of the name of the surgeon who invented it. This explains terms such barbaric probably present on your operating realized or in the mouth of your surgeon.

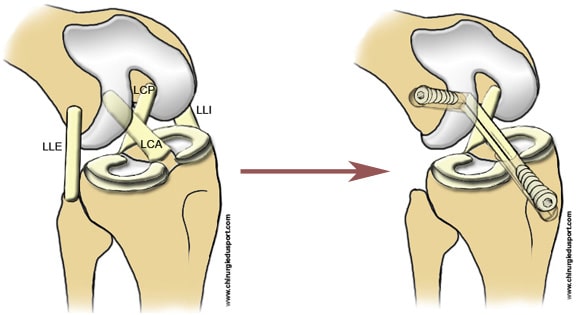
A tendon takes the place of your cruciate ligament. At each of its ends, it is hung in a tunnel in bone.
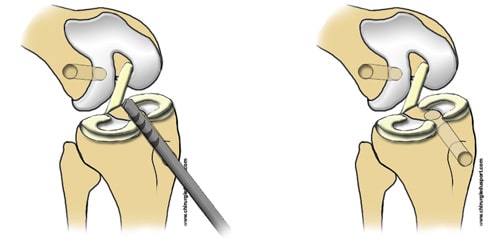
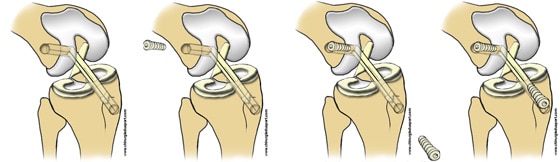
During the operation, it is necessary to drill two holes, one in the bottom of the femur, the other on top of the tibia. Both arrive at the joint where the anterior cruciate cling. In the first tunnel is fixed one end of the tendon taken with a screw. Then you pull up to the second tunnel. Before hanging with another screw, it is tends precisely to ensure maintaining the knee in all positions.
This procedure takes about 1 hour, it involves reconstructing a ligament, which is why it is also called the “ligament”.
The surgeon will also be necessary if the treatment of lesions of the meniscus, cartilage or other ligament.
By looking more closely one ACL, we see that is twisted and consists of two beams. The first is oriented to block the advance of the tibia and the second to limit its rotation. Now, the fineness of surgical techniques allows a “ligament dual beams.” The sampling type “hamstring” including two tendons (Internal Law and Demi Tendinous) lends itself perfectly. Several years of decline and some studies are still lacking for us whether this anatomical reconstruction more effectively protects the knee instability and progressive wear.
Take your daily life, do some physio.
You stay about three days in hospital. You have virtually no evil because anesthetists support your pain. To walk, you use crutches for a few days. Often wearing a brace 2-6 weeks. It aims to protect the anchor points of your new ligament in the bone tunnel. Back at home, you do physical therapy 3-5 times a week. We must recover gradually in joint mobility, regain muscle strength and look of coordination. Your work stoppage is 1 to 3 months. Its duration is often dependent on your ability to perform the journeys. You can easily drive or walk the transport that after two months. Rehabilitation will extend 6 to 8 months! Fortunately, the sport gradually replace it!
Sport is part of your rehabilitation!
A big injury, this is an excellent opportunity to achieve “general physical preparation.” You will return in full form! Take heart! The increase proposed here is the most common evolution. Of course, it varies according to each individual and lesions associated with your cruciate ligament rupture; you must follow the instructions of your surgeon! Upon returning home, doing weight training arms. After 1 month, the rower made by limiting the bending your knee. After this time, it is possible to crawl. But if swimming is easy in a rehabilitation center in a traditional pool, it must pass the floor slippery … Wait 2 months and put your splint to the edge of the basin. At 2 months, you can quietly enjoy the stepper and the bike room. At 3 months, it is possible to pedal more intensively. Simultaneously, start to jog. Four months to begin the real footings.
Slow down ! being Ligamentisation!

Your surgeon has replaced your ligament with a tendon. The first is slightly elastic, the second rather stiff! Progressive mechanical and typically ligament will stimulate the adaptation and transformation of the transplant: the “ligamentisation” But the process is slow and bumpy. Initially, the white blood cells come to reshape the newcomer. It weakens it! Its strength is minimum around 3 to 4 months. No luck, this is the time where you feel much better! You have ants in the feet. In medical parlance it is said that “you too well!” Patience and caution are still needed! Nature must still work to reconstruct a ligament true! For your part, you must persevere to muscle, coordinate and monitor more precisely the movements of your knee. In practice, improving the texture of your transplant supported by increased your physical abilities lets you resume sports with pins and contacts after 6 and 8 months. It’s bad because ligamentisation your tendon is really completes one to two years after surgery.
From 5 months, accelerate and do some lateral movements and changes of direction. Please note, it is programmed gestures and “anticipated” by your brain! Nothing to do with the brutal and uncoordinated movement in response to feint an opponent! At 6 months, group sports practitioners resume technical training but avoid contact. Those who insist on martial arts katas and prohibit fights. Seven months after the procedure, you can train at 100%. Around 8 months, the competition is possible. You must often still a month or two months to find all your automation and “forget” your knee.
to contact us by mail:secretariat@chirurgiedusport.com
Doctor Nicolas LEFEVRE, Doctor Yoann BOHU, Doctor Serge HERMAN, . – 3 janvier 2015.