The diagnosis was made ??by your doctor or sports already confirmed by MRI, it is not urgent to take a surgical decision.
The first three weeks you are immobilized in a splint unarticulated, 20 ° of flexion, you apply ice 30 minutes 3 ??times a day, you are allowed to set foot on the ground.
The following week you find a normal operation without splint. The physiotherapist helps you in this way, gives you a bit of muscle tone and mobility. When the knee is painless and flexible you make an appointment with your sports physician or surgeon of sport to look forward.
What am I going to complain with my knee’s ACL private?
2 definitions before continuing:
- Instability is the dislocation of feeling that you can feel in your knee.
- Laxity is the abnormal movement observed by the physician during the clinical examination of your knee. Laxity can be measured instrumentally radiology (TELOS) or consulting firm (arthrometer).
You may complain of instability, pasdans everyday except rotations (Saturday night dance …), not in the online sports (running, cycling, swimming beat up …) but in sports with pivot or contact (football, skiing, tennis, judo …).
You may complain of pain, not right away, otherwise you should consult your doctor, but in the long run, why?
Because the natural evolution of its private ACL knee to secondary meniscal tears and osteoarthritis is inevitable even in the absence of instability, repeated anterior subluxation of the tibia under the femur (laxity) results.:
- a Progressive relaxation knee holding members (capsule and ligaments)
- Of Meniscal tears and chondral (cartilage) by shearing, almost constant at 10 years, disabling after 25-30 years of evolution (osteoarthritis). You can then complain of pain, instability, effusion, blocking.
A partial lesion was told, possibly cicatrisable ACL!
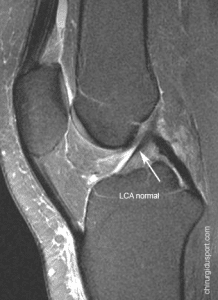
Some clinical signs and imaging give us a little hope of healing: the lack of initial dislocation sensation, lack of initial swelling, laxity tests slightly marked, MRI aspect of LCA tense and vertical. This table specifically justifies the initial capital, the lack of precipitation to surgical repair, and repetition of clinical examination on the knee “cooled” between 6 weeks and 2 months after the accident. The doctor may, if it deems necessary, measure the laxity (or arthrometer TELOS) or request an MRI scan. By cons, whatever MRI appearance of the ACL if the laxity tests are francs therapeutic management is the same as the total rupture.
The total rupture is certain, is it advisable to have surgery?
The natural history of a private ACL knee makes me simplify the therapeutic indications as follows:
- Young-topics, except make arguments against surgery
- Subject> 45 years, does not operate except arguments for surgery
Arguments against surgery:
- Your Knee is stable
- The Laxity tests appreciated by your doctor are weakly positive
- You Are not motivated, you agree to limit yourself to online sports: running, cycling, swimming beats
- You Have a sedentary job
Arguments for surgery:
- You Are unstable
- The Laxity tests are francs
- L’IRM Leaves no doubt as to the complete break-You Are motivated to keep the sports with pivot: football, skiing, tennis …
- You Have a very physical job
I do not have surgery, what precautions I should take?
You have to find a strong knee, well protected by muscle structure that protects it, especially the quadriceps and hamstrings. For this I advise you:
- A Well-conducted rehabilitation, with an isokinetic testing (evaluation of muscle strength test) at the end of rehabilitation
- A Progressive rehabilitation sport starting with bodybuilding and sports online
- A Regular physical maintenance, multi weekly-optionally A knee in sports with pivot or contact.
At the slightest complaint: pain, swelling or instability in the effort, consult your doctor sport.
Total: the doctor informs the patient has.
Doctor Yves GUGLIELMETTI. – 28 janvier 2014.